

Rabies warning, protecting mental health treatment, measles, and a hot World Cup
The CA Dose, June 18, 2026

This week: summer bats and rabies risk, mental health under pressure, a measles milestone, and heated soccer rivalries. We’ll start with bats.
Rabies season is here
As summer approaches, there’s one public health threat most of us don’t think about: rabies. Animal cases peak in the summer, and signs are that it’s ramping up. Last week, San Diego County issued an advisory after recording 14 rabies-positive bats so far this year.
Rabies refresher. Rabies is a viral disease that targets the nervous system. People are infected through saliva of an infected animal, usually through a bite. The virus enters nerve cells at the skin and travels over weeks up to the brain. Symptoms usually appear about 3 to 8 weeks after exposure. Once symptoms begin, theres no treatment, and it’s almost always fatal. But post-exposure vaccination, given promptly after a bite, is highly effective at preventing disease.
Bats. Since January 2024, bats account for 642 (91%) of the 705 animal rabies cases in the state. Skunks are the next most common carriers. Here’s the breakdown of rabies-infected animals reported in California.
Confirmed Rabies Cases by Animal, California
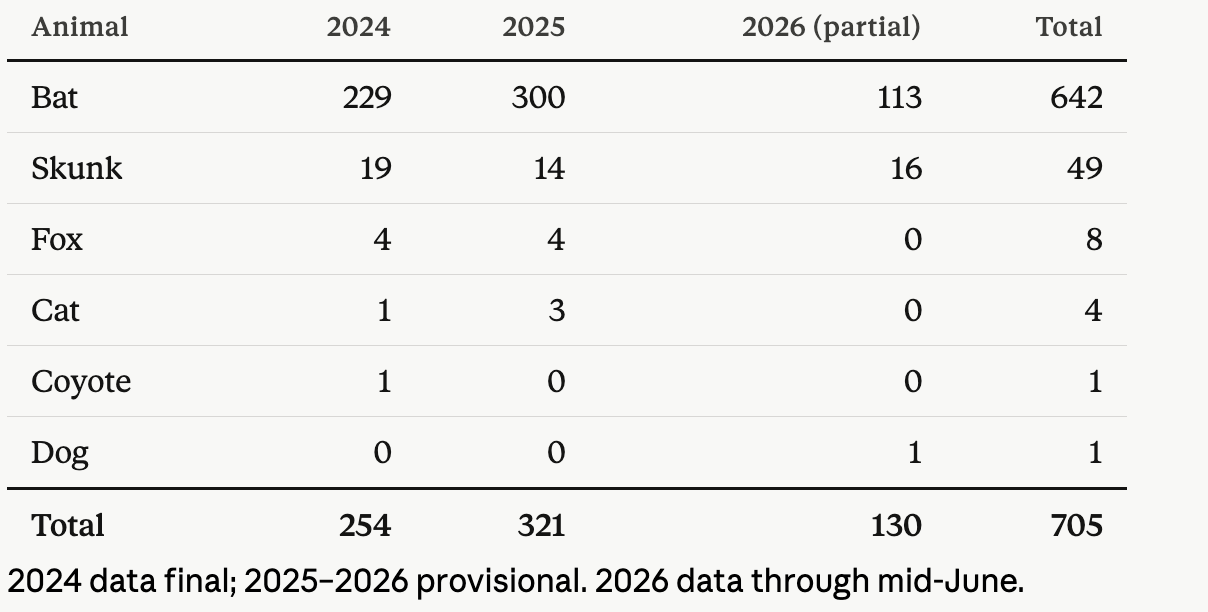
Roughly 10% of bats tested in California are positive for rabies—but that doesn’t mean one in ten bats carry the virus. Healthy bats aren’t interested in people. They work at night and spend their days in dark, hidden spots. Bats we encounter directly have broken from that pattern—the ones we find on the ground in the daytime, or haven’t found their way out of a room are more likely to be sick. We’re testing, and being exposed to, a highly biased sample.
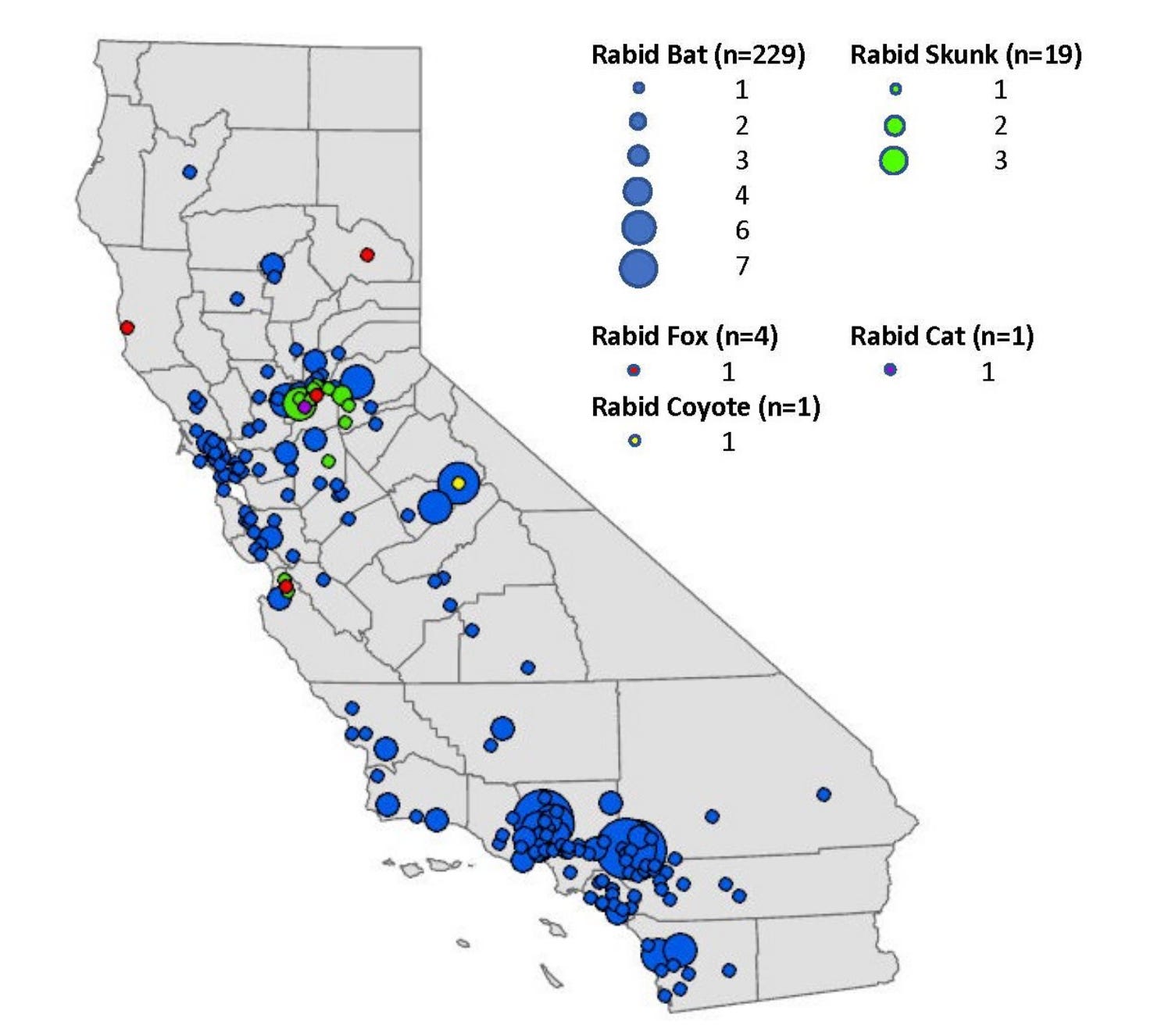
Location of Rabies Cases in Animals: California, 2024
California’s human toll. In November 2024, a Fresno County resident died after being bitten by a bat one month earlier—California’s first human rabies death in over decade. Nationally, deaths from rabies are rare, with fewer than 10 cases each year.
Outside of the U.S. about 70,000 people die annually of rabies, with dogs being the primary carrier. Most cases occur in parts of Africa and Asia which lack the resources for robust rabies prevention programs.
Is there a rabies vaccine? Yes—and it’s used in two ways. Post-exposure protection (PEP) is an emergency series given after a potential exposure. Pre-exposure protection is a two-dose series for people who work directly with animals that could carry rabies—veterinarians, wildlife biologists, animal control officers.
What about my pets? California law requires all dogs be vaccinated, and many cities and counties extend the policy to cats. Vaccinating pets also protects you from an agonizing decision. Under state law, any unvaccinated animal exposed to a suspected rabid animal faces only two options: the animal is put down, or put in a six-month quarantine. A vaccinated pet that is exposed only receives a booster and monitoring. The vaccine is inexpensive, widely available through your vet or humane society, and takes that impossible choice off the table.
What you should do:
Don’t handle bats or wild animals. A bat on the ground, behaving strangely, or active during daylight is a red flag. Call animal control; do not pick it up.
Assume contact if you wake up to a bat in your room. Bat bites can be imperceptible. Discuss post-exposure treatment with a healthcare provider.
Vaccinate your pets. Cats and dogs may have encounters with rabid animals outside of our view, and a vaccine is a highly effective way to keep them healthy.
Wash animal bite wounds immediately with soap and water.
Seek care immediately after any exposure. Post-exposure vaccine is highly effective. There’s no strict window for getting treated, but earlier is better. Once symptoms start, it’s too late.
The West Coast Health Alliance fights again
When the federal government began dismantling vaccine access last year, California, Oregon, Washington, and Hawaii formed the West Coast Health Alliance (WCHA), to protect access to evidence-based standards in our region. The alliance eventually issued independent immunization guidance, which we’ve been following.
Now, the WCHA is stepping up for mental health.
What happened? In May, HHS Secretary Kennedy formally announced a plan to reduce “overprescribing” of psychiatric medications. This followed the report of an FDA panel convened to scrutinize antidepressant use.
The WCHA responded with a statement rejecting federal conclusions, stating that there’s no evidence that psychiatric medications are being overprescribed generally. WCHA asserted that claims about overuse of pharmaceutical treatment reinforces stigma of mental illness and discourages people from seeking care, including medications that may be lifesaving.
Maternal mental health. Avoiding stigma is especially high-stakes during pregnancy—and the federal campaign has made pregnancy a special target. Panelists at the FDA hearing presented unproven theories about links between maternal antidepressant use and autism and fetal alcohol syndrome.

Pregnant people already carry intense cultural pressure to avoid medications; messaging like this only increases that pressure. Depression during pregnancy is associated with maternal mortality, preterm birth, and low birth weight. Recent meta-analyses found no association between prenatal SSRI exposure and risk of birth defects.
Mental health in California. Approximately 5.5 million California adults live with a mental illness. Nearly a third of California adults reported symptoms of anxiety or depression in 2023—and over a third of those who needed mental health care didn’t receive it. Among young Californians who experienced a major depressive episode, approximately 62% received no mental health services at all.
In our recent YLE Pulse survey, only 25% of people believed pregnant people have adequate access to mental health services.
Our challenge in California is the treatment gap—access to care—not the treatments themselves.
Take home: It’s reassuring to see that regional systems can act with consensus to protect us when federal health leadership falters. The WCHA can’t replace federal infrastructure. But as long as Washington is an unreliable source of health information, the West Coast has shown it can hold the line—in protecting access to vaccines, and now, in mental health treatments.
If you or anyone you know is struggling you can call or text 988.
California is free from measles outbreaks. For now.
Sacramento and Placer County just announced the end of the last active measles outbreak in our state, with no new outbreak-related cases in over 42 days. As of June 15, there have been 50 confirmed measles cases in California this year—spread across multiple outbreaks, all eventually contained.
Here’s what that means for us in California.

Sparks coming from outside. This last outbreak began with an unvaccinated traveler returning from South Carolina, where a statewide outbreak was underway. This is our pattern In California: the virus is being introduced, repeatedly, through infections acquired in pockets of low vaccination elsewhere.
I think of it like embers blowing in from a distant fire. We should expect embers to land, but whether they spark a new fire is based on where they land, how dry the vegetation might be, and how quickly they’re recognized and extinguished.
The latest example is a measles case in Santa Clara who visited public places last week—including the international terminal at San Francisco airport—while infectious. The person had returned from travel in an area where measles risk is higher, and brought the virus home.
More than 2,200 confirmed measles cases were reported in the U.S. in 2025. Which means more embers, more often.
California’s buffer. More than 96% of California kindergartners were vaccinated against measles (the measles, mumps rubella, or MMR vaccine) in 2024–25, above the 95% threshold for herd immunity. At the same time, the national average has dropped to 92.5%.
Vaccination rates vary across the state. In 2024–25, 15 of California’s 58 counties reported MMR vaccination rates below 95%. When embers land in these pockets where rates are lower, outbreaks can occur. But, unlike the uncontrolled statewide outbreaks in Utah, Texas, or South Carolina, our outbreaks have been spot-fires that die out, thanks to rapid local public health response and high overall vaccine coverage.
A different kind of reminder. Public health success is often measured in silent, non-events: hospitalizations that didn’t happen, deaths we didn’t experience, outbreaks that don’t spread. It’s one of the reasons public health is under-valued and unseen. But we shouldn’t need to wait for a child to die to be reminded that this matters. Recognizing success in the work we’re doing as communities to protect one another is critical to maintaining it. We’re living with a level of protection that we’ve earned together.
Stay the course. The Sacramento-Placer outbreak is over. But measles will keep arriving. Our job is to keep defenses strong: high coverage, strong response infrastructure, with no illusions that we’re done.
World Cup is heating up
Last week we celebrated an epic Team USA win in Santa Clara. As World Cup rivalries heat up so can the temperature. Heat illness risk increases with large gatherings in the hot sun, if people forget to take precautions.
On opening day, nearly 100 fans fell ill from the heat in Texas, some requiring hospitalization. For every reported heat illness, many more sit just short of emergency, including falls related to dehydration, cardiac problems, kidney stress, and mental status changes in elders.
Keep cool, drink water, know that alcohol and drugs mask heat symptoms, and common medications can increase heat vulnerability. In last week’s post I described how to recognize and avoid heat illness. You can go here to see your heat risk in California this week.
Bottom line
In public health, it’s a challenge to see and call attention to what didn't happen—the bite that didn’t end a life, access to mental health medications, the outbreak that stopped at three cases. But that’s what we do, and it’s worth fighting for.
Love,
Matt
Dr. Matt Willis is the author of Your Local Epidemiologist in California. A California native, he’s served as a primary care physician, CDC epidemiologist, and public health officer for Marin County, where he guided the pandemic response. He lives in Marin with his family and their dogs Teddy and Ramona.
Thank you to Dr. Cynthia He, Vice Chair of the Board of the California State Association of Psychiatrists for her expert contributions to today’s piece on mental health.
I went to veterinary school in the Philippines in the early 80’s. At the time there were more human deaths in the PI than any other countries. We were all vaccinated. There was a study I remember that flushing out human bites wounds prevented rabies transmission from infected animals. Of course I would get post exposure prophylaxis. Just saying we underestimate the value of dilution with infectious disease transmission. Americans seem to feel as if rabies is not a threat to us. How wrong we are.
Hi Matt, hope you’re well. I value the bulletins—keep up the good work!
Agree with Dr Palomo on the value of local wound care, when a bite is recognized! It's the bat exposure without known physical contact recs that I struggle with in terms of public health effectiveness.
According to the abstract of a 2007 report in Clinical Infectious Diseases by De Serres et al., the incidence of human rabies associated with sharing space with bats while sleeping, without known physical contact, was 0.6 cases per billion person-years and there is no evidence that bat-associated rabies incidence has decreased since these ACIP/CDC recs were introduced decades ago. The number needed to treat is astonishingly high, as would be costs, of course.
It's a tough one on an individual level: PEP as a preventive intervention is super-effective and the disease is almost universally fatal, but it's not a compelling use of resources.
Appreciate additional thoughts on this…
Take care
Tom Boo
Eastern Sierra